About OGSIVEO
OGSIVEO is the #1 prescribed and 1st FDA-approved targeted therapy for adult patients with progressing desmoid tumors who require systemic treatment.1
What is OGSIVEO?
OGSIVEO is the #1 prescribed and 1st FDA-approved systemic therapy for adults with progressing desmoid tumors who require systemic treatment.1 OGSIVEO was evaluated in the DeFi study, a Phase 3 pivotal trial that included 142 adult patients with progressing desmoid tumors.2,3
More than 2500 patients have been treated with OGSIVEO in the United States1,*
Reflects commercial patients in the US only. Based on data on file through March 13, 2026.
Desmoid Tumor Treatment Is Evolving
Systemic therapies are recommended as a first-line treatment option for progressive, morbid, or symptomatic desmoid tumors, according to the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) and Desmoid Tumor Working Group (DTWG) Guideline4,5,*
Nirogacestat (OGSIVEO) is recommended as a treatment option by the NCCN Guidelines®
NCCN Guidelines for Soft Tissue Sarcoma recommend nirogacestat (OGSIVEO) as a Category 1 Preferred systemic therapy option for patients with desmoid tumors (aggressive fibromatosis).4
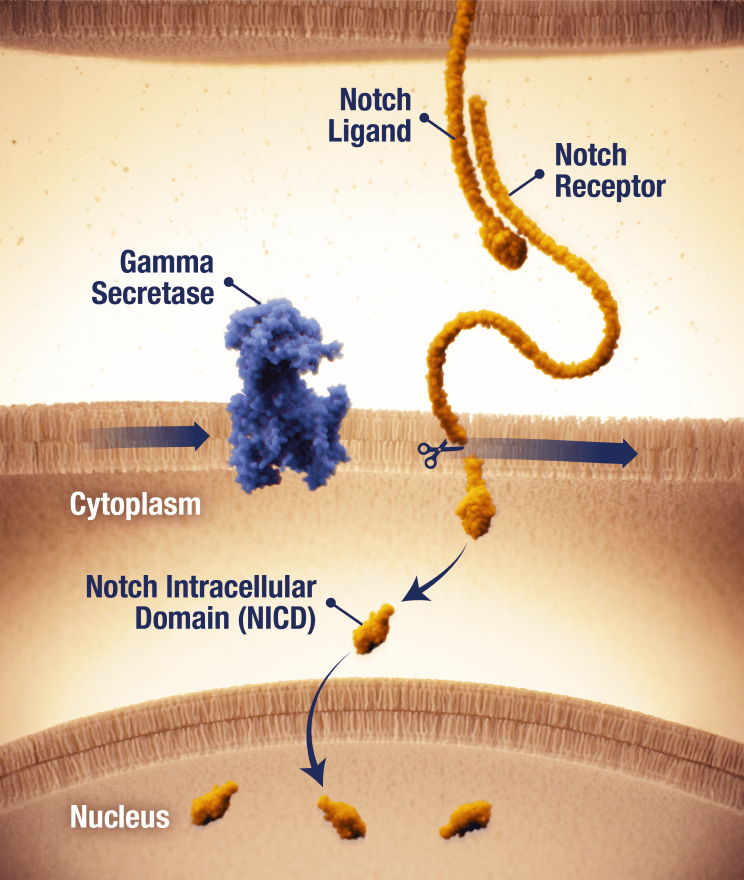
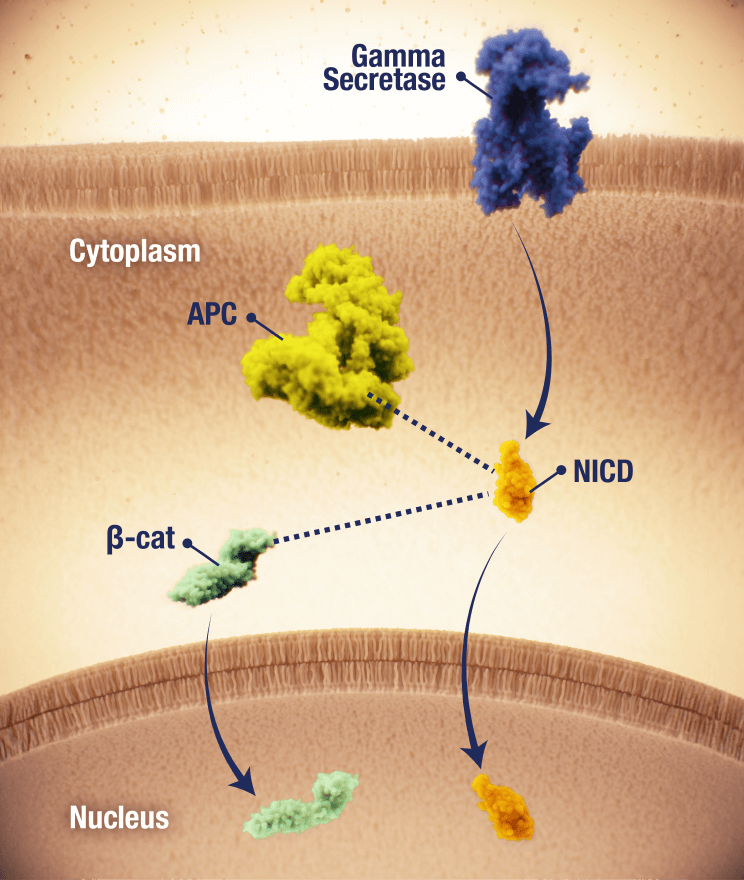
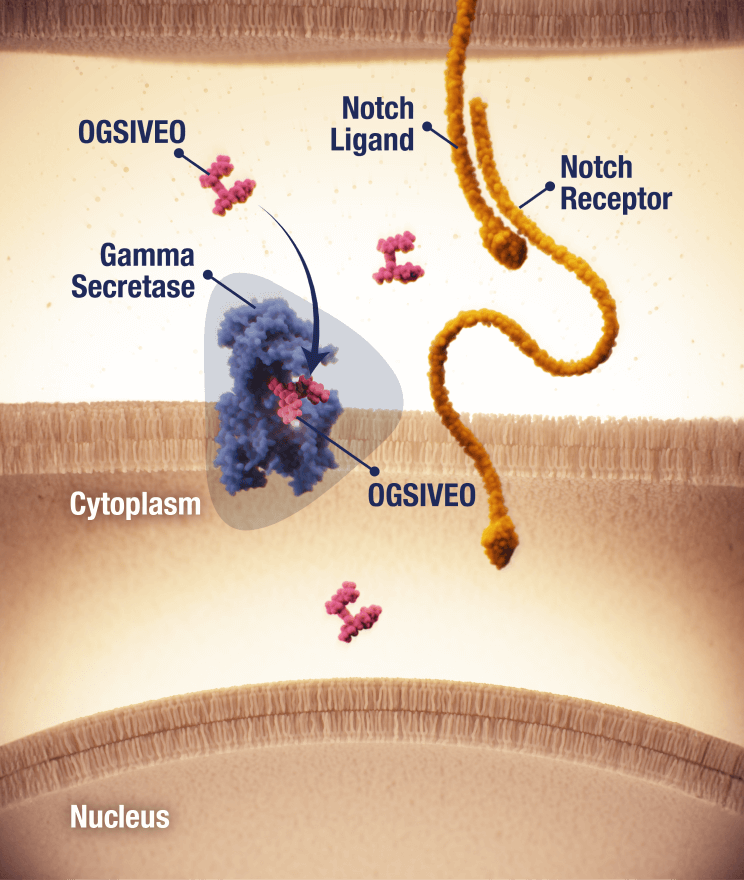
OGSIVEO is the first FDA-approved gamma secretase inhibitor
Proposed mechanism of action based on in vitro models
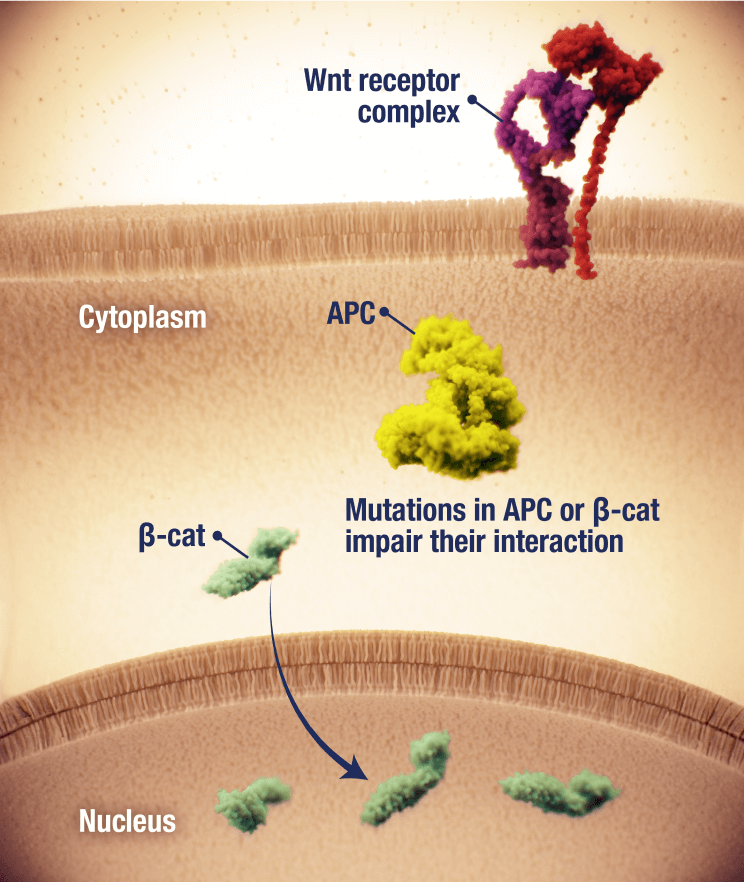
APC, adenomatous polyposis coli; CTNNB1, catenin beta 1; NCCN, National Comprehensive Cancer Network® (NCCN®).
Pivotal Trial Evidence & Long-Term Data
Explore clinical results and long-term data for OGSIVEO.
The DeFi Study Publication
OGSIVEO was evaluated in DeFi—the largest completed Phase 3 trial of an FDA-approved therapy in adult patients with desmoid tumors. Review the results of this landmark study in The New England Journal of Medicine.
Long-term Data Is Available
Explore up to 4 years of data from a long-term post-hoc analysis.2,13
Connect With Us
Sign up to connect with a representative. You can also sign up to receive information and resources directly to your inbox.